
Aotearoa New Zealand enacted an effective response to the Covid-19 pandemic. The government approach to the first few cases in March 2020 was to implement a swift ‘go hard and go early’ response. Borders were closed to non-residents, lockdowns were enforced, and infection was effectively eliminated within 76 days of the first locally acquired case. Although international travel remained heavily restricted, the country enjoyed relative freedom and an open society for many months, while much of the rest of the world struggled to contain rising cases, hospitalisations and fatalities.
The first wave of infection in New Zealand was small, with the majority of the 1503 confirmed or probable cases originating overseas, and just 469 locally acquired cases between February 28th and May 13th 2020. The vast majority of the 1503 cases were from middle to higher income, least deprived groups, reflecting the population of international travellers returning to New Zealand. Locally acquired cases were dominated by 10 superspreader events, involving between 24 and 98 cases, of which four were seeded by international travellers and compounded by large social gatherings.
Life in New Zealand returned to relative normality after the first wave was eliminated, and the period between May 2020 and August 2021 was characterised by long periods of freedom from Covid-19, interspersed by relatively small, well-contained outbreaks. The source of these outbreaks was not always determined, but many were attributed to border incursions and some associated local spread.
New Zealand was buying time, waiting for an effective vaccine to be developed and made available. Infection was controlled until the high rates of transmission associated with the Delta strain could no longer be contained. After failing to eliminate a Delta outbreak, a suppression strategy was adopted in October 2021, augmented by the rollout of the newly available Pfizer vaccine. The de-escalation of control measures resulted in an increase of Delta cases up to the end of 2021, albeit with relatively few fatalities, thanks to good vaccination uptake in the elderly. The Delta outbreak was subsequently dwarfed by the arrival of Omicron early in 2022.

When the pandemic was declared over by the WHO in May 2023, over 2 million cases had been confirmed in New Zealand and over 3000 deaths.
At the whole population level, the response was highly effective, delivering one of the lowest death rates in the world. But how equitable was the response? Did all sectors of New Zealand society enjoy the same experiences, or were some less well served by the government’s response? Given the highly inequitable experiences of indigenous Māori in previous pandemics, such as the 1918-19 flu pandemic - in which Māori experienced a seven-fold higher mortality rate than Europeans - have historical lessons been learned? Most importantly, how do we ensure we have an equitable response to future pandemics?
Aotearoa New Zealand’s unique opportunities and challenges
Aotearoa is a relatively small and isolated archipelago in the South Pacific, with a population of around 5 million that is sparsely populated outside of the main urban centres. This geography immediately brings advantages when preparing for and controlling a pandemic. Borders can be effectively controlled, and transmission contained through national and locally implemented lockdowns and movement restrictions. This undoubtedly prevented uncontrolled border incursions and enabled community transmission to be curtailed for the first 15 months of the pandemic.
In addition, the population was relatively compliant with reasonable, proportionate and clearly justified public health measures. Compliance and organised community responses, particularly in the early stages of the pandemic, enabled non-pharmaceutical interventions to be rolled out and transmission chains to be severed.

The ideal of an equitable response was often discussed in the early stages of the response. However, the centralised response did not lend itself to community-based initiatives or Māori self-determination in decision-making at an operational level (see Box 1).
Box 1: The Aotearoa New Zealand context: Te Tiriti o’ Waitangi (the Treaty of Waitangi) and obligations to indigenous Māori, Pacific peoples and Pacific Realm countries.
There are multiple distinctive characteristics of New Zealand that shaped both the response and the impact of Covid-19. Te Tiriti o Waitangi (the Treaty of Waitangi) is the founding document for New Zealand. It provides an obligation to protect Māori rights, ensuring Māori exercise authority over their affairs. Te Tiriti affirms Māori self-determination in decision-making and requires a partnership with the executive government of New Zealand. This provides protection for Māori and ensures equitable, fair and just outcomes.
Historically, Māori have experienced inequitable wellbeing impacts during pandemics and persistently are underserved by the healthcare system. It is imperative that the principles of Te Tiriti are actively given effect to and applied in the development of future pandemic plans and responses.
During the Covid-19 pandemic, Māori introduced multiple local initiatives in an effort to ensure the safety and protection of their communities. The extensive and highly connected network joined Māori people with their wider community and reinforced partnerships aimed at providing an effective response to the pandemic. In response to multiple outbreaks, Māori partnered, led and delivered effective responses that were key to ensuring the principles of Te Tiriti are given effect and upheld.
Aotearoa New Zealand has a large, diverse, multilingual population of Pacific peoples, with strong and enduring ties to the Pacific Islands and obligations to Pacific countries. The location, demography, community structure, occupations and disproportionate impacts of disease outbreaks on Pacific Peoples all needed to be considered during Covid-19 and preparedness for future pandemics, including engagement of Pacific communities and providers in planning and responses.
Delta, Omicron and inequity. The intent was there, so what went wrong?
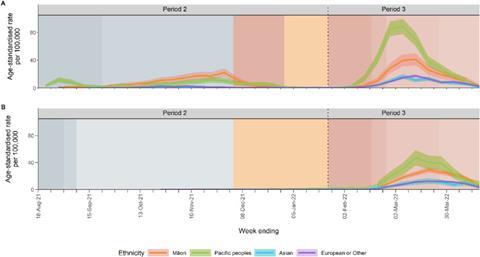
A whole of New Zealand population study investigated whether ethnic health equity was achieved in the response and outcomes, from Covid-19 elimination in June 2020 through to Omicron-response easing, including international border reopening, in 2022.
The findings were stark. Disease outcomes were clearly inequitably distributed. Indigenous Māori and the population of Pacific peoples had markedly higher risks of Covid-19 disease, hospitalisation and death, compared to European and other ethnicities. Vaccines were not equitably distributed; Māori and Pacific populations experienced lower uptake and access, further compounding inequities in the impact of the disease.
The risks of disease were consistently higher across multiple outbreaks, including the Delta and Omicron outbreaks (see Figure 1). The risk of hospitalisation was 2.6 times higher in Māori and 5 times higher in Pacific people compared to Europeans and other ethnicities. A similar pattern was observed for the risk of death.
Why was the response and outcome inequitable? There are many reasons, including:
- The site of incursion: Outbreaks often started at the border. Auckland airport, by far the country’s busiest, has many staff exposed to transmission who were in lower socioeconomic groups, highly connected through ethnicity and community social groups (such as large faith-based groups). The Delta outbreak was linked to an isolation and quarantine facility near Auckland airport. This led to widespread and ultimately uncontrolled transmission, initially overrepresented in the Pacific community and then spreading into the wider Auckland Region, with the highest rates in Māori. The geographical spread of the Delta variant beyond its initial focus around the airport was captured by a detailed analysis of over 3800 genome sequences. This study revealed the importance of both local and long-range spread between communities, and undetected community transmission despite the implementation of stringent lockdown measures.
- Risk factors for community transmission: Some of the most affected groups lived in crowded housing, exacerbating transmission. These groups often tended to have relatively high rates of employment in public-facing sectors such as hospitality, roles where remote work is not possible, and insecure employment conditions. Furthermore, the same communities, including Māori and Pacific populations, have higher rates of comorbidity and multi-morbidity, putting them at higher risk of severe illness from Covid-19.
- Lack of support for community -based initiatives: The centralised, top-down design of pandemic control measures meant that they often did not align with the values or lived realities of more marginalised populations.
- Inequitable distribution and uptake of vaccines compounded inequitable disease outcomes. Despite recommendations to explicitly prioritise Māori and Pacific ethnic groups for vaccination, the government chose a primarily age-prioritised vaccine rollout. Because Māori and Pacific populations are younger than those of European ethnicity, they were effectively put at the back of the vaccine queue. This allowed more time for anti-vaccination rhetoric and disinformation to take hold in these groups.
”The uneven impact of the pandemic was nothing new, but rather the continuation of a long history of health inequities stemming from colonisation and systemic racism. Pandemics will generally exacerbate pre-existing inequities, and this is exactly what happened with Covid-19.”
The best pandemic response in the world is not going to make existing inequities disappear. This means that we need sustained investment in improving health outcomes for Māori and Pacific populations before the next pandemic arrives. Leveraging the strength of these communities, supporting trusted healthcare providers and community initiatives, and enhancing opportunities for collaboration will help increase preparedness while mitigating predictable negative outcomes.

The need to develop models that explicitly consider Māori and Pacific people
Models were used throughout the pandemic in New Zealand to inform national policy. Modelling is not a crystal ball, and it can’t tell you what to do, but it can help understand the likely future trajectory of the pandemic and how that might change under different interventions. For example, models were used to estimate the risk of border-related outbreaks, understand the impact of vaccination, and navigate reopening decisions. Overall, models were one source of evidence that supported informed decision-making.
Although models played an important role in supporting New Zealand’s response to Covid-19, they were limited in their ability to quantify inequities in disease impact between different population groups, for example, different ethnicities. The next generation of models needs to account for the dynamic interaction between disease transmission and social, economic and cultural factors. These factors intersect in complex ways. For example, large household size, multi-generational households and inability to work from home contribute to greater exposure to infection. Access to healthcare services and exposure to misinformation affect vaccine uptake. Comorbidities and pre-existing inequities in health outcomes affect disease severity.
Disentangling the relative contributions of factors like these is a challenge for modellers, and requires both methodological advances in modelling techniques as well as better-quality data to inform and validate models. Modellers also need to strike a delicate balance between capturing fine-grained detail and avoiding overly complex models. The aphorism that models should be “as simple as possible, but no simpler” is particularly relevant when the need to be deployed in real time and communicated succinctly to policymakers. However, as the pandemic laid bare, ignoring inequities that are both predictable and preventable is not going to help support an equitable public health response.

Conclusions – the way forward
Overall, New Zealand’s response to Covid-19 was successful. New Zealand experienced relatively low excess mortality, and the economy was less impacted compared to other countries. However, looking beyond the country-level data reveals stark inequities in access to vaccination and Covid-19 outcomes that need to be addressed for future planning.
Two public inquiries have been held. These have made a series of recommendations, several of which specifically refer to addressing inequity in the country’s response. A Pandemic Strategic Framework is being drawn up in the wake of these inquiries. This covers a range of initiatives from updating legislation to reviewing our reserve supply of medicine and equipment for emergencies and aims to set the direction for the country’s approach to pandemic prevention, preparedness and response.
Policies are needed to address disparities in the upstream determinants of inequitable outcomes. Vaccine programme planning and implementation needs to be carried out in partnership with high-risk communities, and the prioritisation process needs to address systematic ethnic disadvantage and promote health equity in response decision-making.
The development of the Pandemic Strategic Framework is part of a broader initiative, the National Risk and Resilience Framework, and aligns with objectives in the Government Policy Statement on Health. If successful, it will help to prevent and respond equitably to future pandemics and other major health security threats by ensuring New Zealand has sufficient capacity, capability, and infrastructure in place, and the necessary partnerships with more vulnerable communities.
The experiences of the Covid-19 pandemic must be learned from and incorporated into future preparedness, planning and response. If they are not, history will repeat itself again, and the same inequities will be realised in future pandemics.



No comments yet