Chikungunya fever, caused by Chikungunya virus (CHIKV), has re‑emerged as a major global health threat. The 2025 outbreak in Guangdong, China – the largest local epidemic ever recorded – marks a critical epidemiological turning point.
While conventional care remains supportive, traditional Chinese medicine (TCM) offers complementary strategies for acute symptoms and chronic polyarthralgia. This review synthesizes current knowledge on etiology, pathogenesis, clinical features, and management, with emphasis on evidence‑based TCM integration.
It concludes that a multipronged public health approach, combining standard measures with validated TCM therapies, is essential, and calls for rigorous clinical trials to globalize these integrative treatments.
MICROBIOLOGY NEWS: Register with The Microbiologist for more free articles
CHIKV is an alphavirus transmitted by Aedes mosquitoes. First identified in Tanzania in 1952, it has now spread to over 119 countries. Viral adaptations have expanded vector competence, enabling temperate‑zone transmission.
The July 2025 Foshan outbreak – over 4,000 confirmed cases – signifies a shift from sporadic imported cases to sustained local transmission in China, highlighting vulnerabilities in naive populations. Conventional management is symptomatic, but TCM integration shows promise, forming the focus of this review.
Etiology and viral replication
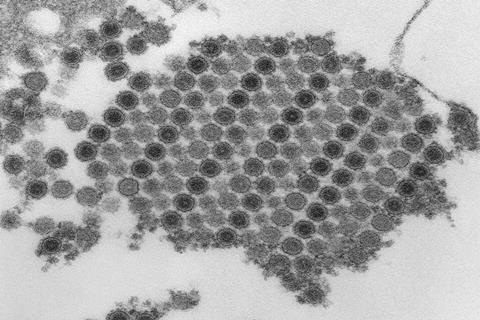
CHIKV is an enveloped, positive‑sense RNA virus with an ~11.8‑kb genome. Two ORFs encode non‑structural (Nsp1‑4) and structural (C, E1, E2) proteins. Four genotypes exist; the East/Central/South African (ECSA) genotype drives current outbreaks, with mutations potentially linked to chronic arthritis. Viral entry involves E2 binding to receptors like MXRA8, endocytosis, pH‑dependent fusion, and cytoplasmic replication. New virions bud from the host cell surface, completing the cycle.
Pathogenesis involves direct cytopathic effects and a dysregulated immune response. After skin replication, the virus disseminates to joints, muscles, and other organs. Strong innate immunity – type I interferons and pro‑inflammatory cytokines (IL‑1β, IL‑6) – controls virus but also recruits immune cells, causing tissue damage and arthralgia. CD8⁺ T cells may become exhausted. Chronic polyarthralgia arises from persistent viral RNA/antigens in tissue reservoirs and/or a virus‑triggered autoimmune‑like reaction. IL‑6‑driven osteoclastogenesis further contributes to bone erosion.
MICROBIOLOGY ON TAP: Get full access to all The Microbiologist articles from just £2.17 a month
The disease has three phases: acute (14–21 days) with sudden high fever, rash, and severe symmetric polyarthralgia (distal joints); subacute (up to 3 months) with persisting joint symptoms; and chronic (>3 months) in 40–80% of patients, causing long‑term morbidity. Mortality is low, but severe complications (neurological, cardiac, ocular) can occur in neonates, elderly, and comorbid individuals. Differential diagnosis from dengue and Zika relies on features like thrombocytopenia (dengue), severe arthralgia (chikungunya), and pruritus (Zika).
Therapeutic and preventive strategies
No specific antivirals exist. Acute phase management includes rest, hydration, and acetaminophen; severe pain may need opioids, but corticosteroids are avoided. Chronic phase uses NSAIDs, low‑dose corticosteroids, or DMARDs (methotrexate, hydroxychloroquine), plus physiotherapy.
TCM integration is officially recommended in China’s 2025 national protocol. Based on “dampness‑heat” theory: (1) Acute phase – “clearing heat, resolving dampness” with herbs like Guanghuoxiang, Gegen, Lianqiao; (2) Recovery phase – “dispelling cold and removing dampness” for persistent arthralgia using Qianghuo, Duhuo, Qinjiao; (3) External therapies – bloodletting at acupoints or joints, and cold herbal compresses (Rendongteng) for local relief. However, high‑quality international evidence is limited, demanding rigorous trials.
Prevention benefits from two newly approved vaccines (Ixchiq for ≥18 years; Vimkunya for ≥12 years), though safety, cost, and equitable access remain challenges. Integrated vector control (source reduction, insecticides, Wolbachia‑infected mosquitoes) remains fundamental.
Outlook and challenges
Future priorities include: (1) unraveling chronic arthralgia mechanisms and developing predictive biomarkers; (2) ensuring vaccine equity, regional reserves, and post‑licensure surveillance; (3) advancing affordable therapies, including TCM with molecular target studies. Current research gaps include insufficient TCM mechanistic data, lack of vaccine trials in low‑income countries, and small sample sizes in long‑term follow‑up studies.
A holistic response to CHIKV requires combining clinical surveillance, environmental monitoring, cross‑border collaboration, and community engagement, alongside standard care and evidence‑based TCM. Strengthened global cooperation and research investment will enhance preparedness and reduce the impact of this growing arboviral threat.
The study was recently published in the Future Integrative Medicine.






{kind=link}
No comments yet