The long-term clinical outcomes of patients with hepatitis B virus (HBV)-related cirrhosis receiving nucleos(t)ide analog (NA) therapy according to virological response patterns remain inadequately defined. A new study aimed to investigate the association between virological response patterns and clinical outcomes in a large, long-term, real-world cohort.
This retrospective–prospective cohort study enrolled patients with HBV-related cirrhosis receiving NA therapy from 2009 to 2019. According to the serum HBV DNA levels during the initial two years of antiviral treatment, patients were categorized as having a complete (CVR) or partial virological response (PVR).
Patients with CVR were further stratified according to their dynamic HBV DNA changes during follow-up into maintained virological response (MVR) or virological breakthrough (VBT) patterns.
The primary clinical outcomes included hepatocellular carcinoma (HCC), acute-on-chronic liver failure, and liver-related death. Secondary endpoints included recompensation and progression to decompensation. Cox proportional hazards regression was used to assess the association between virological response patterns and clinical endpoints.
The findings
In total, 1,869 patients were enrolled. During a median follow-up of seven years, the MVR, VBT, and PVR rates were 65.4%, 26.5%, and 8.1%, respectively. The cumulative serum hepatitis B surface antigen (HBsAg) clearance rate was 9.8%. Moreover, 34.9% of patients with HBsAg < 100 IU/mL at baseline experienced HBsAg clearance.
Compared with patients with VBT and PVR, those with MVR had a lower five- and ten-year cumulative incidence of HCC in both the compensated (five-year: 10.1% vs. 17.0%; ten-year: 14.2% vs. 33.6%; P < 0.001) and decompensated cirrhosis subgroups (five-year: 19.5% vs. 36.7%; ten-year: 25.7% vs. 49.7%; P < 0.001).
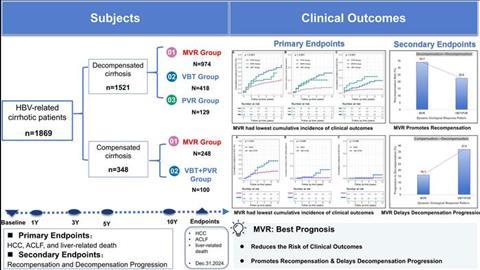
Similarly, patients with MVR also had a lower cumulative incidence of liver-related death. Additionally, a higher hepatic recompensation rate was observed in patients with MVR than in those with VBT (34.1% vs. 22.5%, P < 0.001). Importantly, patients achieving HBsAg clearance and undetectable serum HBV DNA levels (“functional cure” during ongoing NA therapy) had the lowest five- and ten-year cumulative incidence of HCC (3.9% and 8.7%, respectively).
Conclusions
Patients with a long-term MVR pattern had a lower incidence of HCC and liver-related death in both compensated and decompensated HBV-related cirrhosis subgroups, especially among patients achieving “functional cure.”
Among patients with decompensated cirrhosis at baseline, those who experienced MVR had a higher hepatic recompensation rate than those who experienced VBT or PVR. Similarly, among patients with compensated cirrhosis at baseline, those with MVR had a lower rate of progression to decompensation.
However, more than 30% of patients experienced PVR or VBT during long-term NA therapy. These findings highlight the importance of rigorous monitoring and risk stratification for patients at high risk of HCC after initial CVR to optimize outcomes and guide clinical decisions. This potential benefit in improving clinical outcomes lies in optimizing salvage therapy and strengthening HCC monitoring in accordance with current guidelines for patients with PVR or VBT.
The study was recently published in the Journal of Clinical and Translational Hepatology.






No comments yet